中国临床药理学与治疗学 ›› 2026, Vol. 31 ›› Issue (6): 851-864.doi: 10.12092/j.issn.1009-2501.2026.06.015
• 药物治疗学 • 上一篇
程紫萍1,2( ), 查娴1,*()
), 查娴1,*()
收稿日期:2025-07-01
出版日期:2026-06-26
发布日期:2026-07-06
通讯作者:
查娴
E-mail:1079951505@qq.com;zxyzx0702@163.com
作者简介:程紫萍,女,硕士,初级药师,研究方向:临床药学。E-mail:基金资助:
Ziping CHENG1,2(), Xian ZHA1,*()
Received:2025-07-01
Online:2026-06-26
Published:2026-07-06
Contact:
Xian ZHA
E-mail:1079951505@qq.com;zxyzx0702@163.com
摘要:
目的: 探讨头孢他啶/阿维巴坦(ceftazidime-avibactam,CZA)单药与联合用药方案在治疗重症患者耐碳青霉烯类革兰阴性杆菌(carbapenem resistant organism,CRO)感染中的临床疗效,并分析影响预后的危险因素。方法: 研究纳入了2019年9月1日至2023年12月31日期间在东南大学附属中大医院住院治疗的96例CRO感染患者。根据治疗方案,将患者分为单药组(59例)和联用组(37例)。采用倾向性评分匹配(propensity score matching,PSM)方法对两组患者进行匹配,以减少基线差异。主要结局指标包括30天全因死亡率、30天临床治愈率,次要结局指标包括14天全因死亡率、微生物清除率、总住院时间、重症医学科(intensive care unit,ICU)住院时间、机械通气时间。结果: 倾向性评分匹配后共纳入74名患者,其中单药组37例,联用组37例。单药组倾向性评分匹配前30天全因死亡率为35.6%,联用组为21.6%,倾向性评分匹配后两组分别为40.5%和21.6%,匹配前后差异无统计学意义(P=0.147,P=0.079);倾向性评分匹配前30天临床治愈率单药组和联用组分别为62.7%和73.0%,匹配后两组分别为56.8%和73.0%,匹配前后差异均无统计学意义(P=0.299,P=0.144)。然而,联用组的微生物清除率显著高于单药组(70.3% vs. 49.2%,P=0.042),倾向性评分匹配后结果仍保持稳定(P=0.010)。两组14天全因死亡率、机械通气时间、ICU住院时间以及总住院时间均无统计学差异(P>0.05)。多因素Logistic回归分析显示,使用血管活性药物、高龄是增加CRO感染患者30天全因死亡率的独立危险因素(P<0.05);高龄、培养阳性至用药间隔久、糖尿病是降低微生物清除率的独立危险因素,而联合用药是显著提高微生物清除率的有利因素(P<0.05)。结论: 尽管联合用药方案并未在降低CRO感染患者30天全因死亡率和提高30天临床治愈率等方面体现出显著优势,但联合用药组具有更高的微生物清除率。本研究结果为CZA在CRO感染治疗中的应用提供了新的临床证据。
中图分类号:
程紫萍, 查娴. 头孢他啶/阿维巴坦治疗重症患者耐碳青霉烯革兰阴性杆菌的临床疗效分析[J]. 中国临床药理学与治疗学, 2026, 31(6): 851-864.
Ziping CHENG, Xian ZHA. Clinical efficacy of ceftazidime/avibactam in critically ill patients with carbapenem-resistant gram-negative organism infections[J]. Chinese Journal of Clinical Pharmacology and Therapeutics, 2026, 31(6): 851-864.
| Characteristics | Before propensity score matching | After propensity score matching | |||||
| Monotherapy group (n=59) | Combination therapy group (n=37) | P value | Monotherapy group (n=37) | Combination therapy group (n=37) | P value | ||
| Age[M(P25, P75)] | 72(57,80) | 67(49,75) | 0.046* | 68(55,78.5) | 67(49,75) | 0.272 | |
| BMI (x?±s) | 22.90±3.68 | 23.05±2.87 | 0.837 | 23.24±3.90 | 23.04±2.87 | 0.805 | |
| SOFA[M(P25, P75)] | 7.0(4,10) | 8.0(3.5,11) | 0.587 | 7.3(3,11.6) | 7.8(3,12.6) | 0.612 | |
| APACHE Ⅱ[M(P25, P75)] | 19(13,24) | 17(14,23.5) | 0.541 | 22(15,23.5) | 17(14,23.5) | 0.309 | |
| Male [n(%)] | 43(72.9) | 32(86.5) | 0.117 | 29(78.4) | 32(86.5) | 0.359 | |
| Hours from admission to culture collection[M(P25, P75)] | 48(8.5,96) | 48(24,96) | 0.477 | 72(24,108) | 48(24,96) | 0.811 | |
| Medication course[M(P25, P75)] | 11 (7,14) | 11(9,14.5) | 0.287 | 11(7,14) | 11(9,14.5) | 0.332 | |
| Comorbidities[n(%)] | |||||||
| Hypertension | 17(28.8) | 7(18.9) | 0.276 | 10(27) | 7(18.9) | 0.407 | |
| Diabetes | 21(35.6) | 5(13.5) | 0.018* | 8(21.6) | 5(13.5) | 0.359 | |
| Malignancy | 6(10.2) | 6(16.2) | 0.579 | 4 (10.8) | 6(16.2) | 0.496 | |
| Cardiovascular disease | 25(42.4 | 15(40.5) | 0.859 | 16(43.2) | 15(40.5) | 0.814 | |
| Liver disease | 17(28.8) | 13(35.1) | 0.515 | 11(29.7) | 13(35.1) | 0.619 | |
| Kidney disease | 36(61.0) | 27(73.0) | 0.230 | 27(73.0) | 27(73.0) | 1.000 | |
| COPD | 4(6.8) | 2(5.4) | 1.000 | 4(10.8) | 2(5.4) | 0.670 | |
| ARDS | 21(35.6) | 12(32.4) | 0.751 | 13(35.1) | 12(32.4) | 0.806 | |
| Severity of illness [n(%)] | |||||||
| CRRT | 16(27.1) | 12(32.4) | 0.577 | 13(35.1) | 12(32.4) | 0.806 | |
| Multisite infections | 24(40.7) | 21(56.8) | 0.124 | 16(43.2) | 21(56.8) | 0.245 | |
| Usage of vasoactive agent | 35(59.3) | 23(62.2) | 0.782 | 21(56.8) | 23(62.2) | 0.636 | |
| Septic shock | 42(71.2) | 22(59.5) | 0.236 | 24(64.9) | 22(59.5) | 0.632 | |
| Infection sites[n(%)] | |||||||
| Bloodstream | 16(27.1) | 19(51.4) | 0.016* | 12(32.4) | 19(51.4) | 0.099 | |
| Urine | 14(23.7) | 7(18.9) | 0.579 | 9(24.3) | 7(18.9) | 0.572 | |
| Abdominal | 9(15.0) | 7(18.9) | 0.613 | 4(10.8) | 7(18.9) | 0.327 | |
| Lung | 47(79.7) | 28(75.7) | 0.646 | 29(78.4) | 28(75.7) | 0.782 | |
| Skin | 3(5.1) | 1(2.7) | 0.965 | 1(2.7) | 1(2.7) | 1.000 | |
| Intracranial | 2(3.4) | 2(5.4) | 1.000 | 2(5.4) | 2(5.4) | 1.000 | |
表 1
Table 1 Clinical characteristics of patients with CRO infections in the monotherapy group and combination therapy group
| Characteristics | Before propensity score matching | After propensity score matching | |||||
| Monotherapy group (n=59) | Combination therapy group (n=37) | P value | Monotherapy group (n=37) | Combination therapy group (n=37) | P value | ||
| Age[M(P25, P75)] | 72(57,80) | 67(49,75) | 0.046* | 68(55,78.5) | 67(49,75) | 0.272 | |
| BMI (x?±s) | 22.90±3.68 | 23.05±2.87 | 0.837 | 23.24±3.90 | 23.04±2.87 | 0.805 | |
| SOFA[M(P25, P75)] | 7.0(4,10) | 8.0(3.5,11) | 0.587 | 7.3(3,11.6) | 7.8(3,12.6) | 0.612 | |
| APACHE Ⅱ[M(P25, P75)] | 19(13,24) | 17(14,23.5) | 0.541 | 22(15,23.5) | 17(14,23.5) | 0.309 | |
| Male [n(%)] | 43(72.9) | 32(86.5) | 0.117 | 29(78.4) | 32(86.5) | 0.359 | |
| Hours from admission to culture collection[M(P25, P75)] | 48(8.5,96) | 48(24,96) | 0.477 | 72(24,108) | 48(24,96) | 0.811 | |
| Medication course[M(P25, P75)] | 11 (7,14) | 11(9,14.5) | 0.287 | 11(7,14) | 11(9,14.5) | 0.332 | |
| Comorbidities[n(%)] | |||||||
| Hypertension | 17(28.8) | 7(18.9) | 0.276 | 10(27) | 7(18.9) | 0.407 | |
| Diabetes | 21(35.6) | 5(13.5) | 0.018* | 8(21.6) | 5(13.5) | 0.359 | |
| Malignancy | 6(10.2) | 6(16.2) | 0.579 | 4 (10.8) | 6(16.2) | 0.496 | |
| Cardiovascular disease | 25(42.4 | 15(40.5) | 0.859 | 16(43.2) | 15(40.5) | 0.814 | |
| Liver disease | 17(28.8) | 13(35.1) | 0.515 | 11(29.7) | 13(35.1) | 0.619 | |
| Kidney disease | 36(61.0) | 27(73.0) | 0.230 | 27(73.0) | 27(73.0) | 1.000 | |
| COPD | 4(6.8) | 2(5.4) | 1.000 | 4(10.8) | 2(5.4) | 0.670 | |
| ARDS | 21(35.6) | 12(32.4) | 0.751 | 13(35.1) | 12(32.4) | 0.806 | |
| Severity of illness [n(%)] | |||||||
| CRRT | 16(27.1) | 12(32.4) | 0.577 | 13(35.1) | 12(32.4) | 0.806 | |
| Multisite infections | 24(40.7) | 21(56.8) | 0.124 | 16(43.2) | 21(56.8) | 0.245 | |
| Usage of vasoactive agent | 35(59.3) | 23(62.2) | 0.782 | 21(56.8) | 23(62.2) | 0.636 | |
| Septic shock | 42(71.2) | 22(59.5) | 0.236 | 24(64.9) | 22(59.5) | 0.632 | |
| Infection sites[n(%)] | |||||||
| Bloodstream | 16(27.1) | 19(51.4) | 0.016* | 12(32.4) | 19(51.4) | 0.099 | |
| Urine | 14(23.7) | 7(18.9) | 0.579 | 9(24.3) | 7(18.9) | 0.572 | |
| Abdominal | 9(15.0) | 7(18.9) | 0.613 | 4(10.8) | 7(18.9) | 0.327 | |
| Lung | 47(79.7) | 28(75.7) | 0.646 | 29(78.4) | 28(75.7) | 0.782 | |
| Skin | 3(5.1) | 1(2.7) | 0.965 | 1(2.7) | 1(2.7) | 1.000 | |
| Intracranial | 2(3.4) | 2(5.4) | 1.000 | 2(5.4) | 2(5.4) | 1.000 | |
| Clinical outcome | Before propensity score matching | After propensity score matching | |||||
| Monotherapy group (n=59) | Combination therapy group (n=37) | P value | Monotherapy group (n=37) | Combination therapy group (n=37) | P value | ||
| Primary outcomes | |||||||
| 30-day all-cause mortality [n(%)] | 21(35.6) | 8(21.6) | 0.147 | 15(40.5) | 8(21.6) | 0.079 | |
| 30-day clinical response [n(%)] | 37(62.7) | 27(73.0) | 0.299 | 21(56.8) | 27(73.0) | 0.144 | |
| Secondary outcomes | |||||||
| 14-day all-cause mortality [n(%)] | 17(28.8) | 8(21.6) | 0.435 | 12(32.4) | 8(21.6) | 0.295 | |
| Microbiological clearance[n(%)] | 29(49.2) | 26(70.3) | 0.042* | 15(40.5) | 26(70.3) | 0.010* | |
| Duration of mechanical ventilation (days) [M(P25, P75)] | 13(6,29) | 19(9.5,30) | 0.381 | 15(6.5,32) | 19(9.5,30) | 0.618 | |
| Length of ICU stay (days) [M(P25, P75)] | 22 (12,37) | 25(18,52.5) | 0.119 | 22 (12,35) | 25(18,52.5) | 0.211 | |
| Length of hospital stay (days) [M(P25, P75)] | 32(20,54) | 46(27.5,76.5) | 0.031* | 32(21.5,52.5) | 46(27.5,76.5) | 0.057 | |
表 2
Table 2 Clinical outcomes of the study patients
| Clinical outcome | Before propensity score matching | After propensity score matching | |||||
| Monotherapy group (n=59) | Combination therapy group (n=37) | P value | Monotherapy group (n=37) | Combination therapy group (n=37) | P value | ||
| Primary outcomes | |||||||
| 30-day all-cause mortality [n(%)] | 21(35.6) | 8(21.6) | 0.147 | 15(40.5) | 8(21.6) | 0.079 | |
| 30-day clinical response [n(%)] | 37(62.7) | 27(73.0) | 0.299 | 21(56.8) | 27(73.0) | 0.144 | |
| Secondary outcomes | |||||||
| 14-day all-cause mortality [n(%)] | 17(28.8) | 8(21.6) | 0.435 | 12(32.4) | 8(21.6) | 0.295 | |
| Microbiological clearance[n(%)] | 29(49.2) | 26(70.3) | 0.042* | 15(40.5) | 26(70.3) | 0.010* | |
| Duration of mechanical ventilation (days) [M(P25, P75)] | 13(6,29) | 19(9.5,30) | 0.381 | 15(6.5,32) | 19(9.5,30) | 0.618 | |
| Length of ICU stay (days) [M(P25, P75)] | 22 (12,37) | 25(18,52.5) | 0.119 | 22 (12,35) | 25(18,52.5) | 0.211 | |
| Length of hospital stay (days) [M(P25, P75)] | 32(20,54) | 46(27.5,76.5) | 0.031* | 32(21.5,52.5) | 46(27.5,76.5) | 0.057 | |
| Pathogen | Infection source | n | Proportion |
| Klebsiella pneumoniae | 91 | 81.25% | |
| Lung | 36 | 32.14% | |
| Abdominal | 9 | 8.04% | |
| Urine | 14 | 12.50% | |
| Skin | 2 | 1.79% | |
| Bloodstream | 27 | 24.11% | |
| Intracranial | 3 | 2.68% | |
| Pseudomonas aeruginosa | 17 | 15.18% | |
| Lung | 15 | 13.39% | |
| Abdominal | 1 | 0.89% | |
| Urine | 1 | 0.89% | |
| Escherichia coli | Urine | 1 | 0.89% |
| Hoffmann's enterobacterium | Intracranial | 1 | 0.89% |
| Enterobacter cloacae | Abdominal | 1 | 0.89% |
| Serratia marcescens | Bloodstream | 1 | 0.89% |
表 3
Table 3 Characteristics of CRO isolates from patients
| Pathogen | Infection source | n | Proportion |
| Klebsiella pneumoniae | 91 | 81.25% | |
| Lung | 36 | 32.14% | |
| Abdominal | 9 | 8.04% | |
| Urine | 14 | 12.50% | |
| Skin | 2 | 1.79% | |
| Bloodstream | 27 | 24.11% | |
| Intracranial | 3 | 2.68% | |
| Pseudomonas aeruginosa | 17 | 15.18% | |
| Lung | 15 | 13.39% | |
| Abdominal | 1 | 0.89% | |
| Urine | 1 | 0.89% | |
| Escherichia coli | Urine | 1 | 0.89% |
| Hoffmann's enterobacterium | Intracranial | 1 | 0.89% |
| Enterobacter cloacae | Abdominal | 1 | 0.89% |
| Serratia marcescens | Bloodstream | 1 | 0.89% |
| Risk factors | 30 d survival (n=51) | 30 d mortality (n=23) | P value |
| Basic characteristics | |||
| Age[M(P25, P75)] | 64(46,76) | 71(67,77) | 0.036* |
| BMI[M(P25, P75)] | 22.86(20.81,25.46) | 22.86(20.28,23.88) | 0.139 |
| SOFA[M(P25, P75)] | 6(3,10) | 10(7,12) | 0.001* |
| APACHE Ⅱ[M(P25, P75)] | 17(13,22) | 23(19,26) | <0.001* |
| Male | 44(86.3) | 17(73.9) | 0.335 |
| Medication course[M(P25, P75)] | 11(9,16) | 11(6,14) | 0.064 |
| Combination therapy[M(P25, P75)] | 29(56.9) | 8(34.8) | 0.079 |
| Comorbidities[n(%)] | |||
| Hypertension | 14(27.5) | 3(13.0) | 0.173 |
| Diabetes | 8(15.7) | 5(21.7) | 0.762 |
| COPD | 5(9.8) | 1(4.3) | 0.737 |
| Cardiovascular disease | 23(45.1) | 8(34.8) | 0.405 |
| Malignancy | 7(13.7) | 3(13.0) | 1.000 |
| Liver disease | 14(27.5) | 10(43.5) | 0.173 |
| Kidney disease | 35(68.5) | 19(82.6) | 0.210 |
| ARDS | 12(23.5) | 13(56.5) | 0.005* |
| Severity of illness[n(%)] | |||
| Multisite infections | 25(49.0) | 12(52.2) | 0.802 |
| Septic shock | 26(51.0) | 20(87.0) | 0.003* |
| Usage of vasoactive agent | 24(47.1) | 20(87.0) | 0.001* |
| CRRT | 13(25.5) | 12(52.2) | 0.025* |
| Hours from admission to culture[M(P25, P75)] | 48(24,96) | 48(24,144) | 0.449 |
| Infection sites[n(%)] | |||
| Bloodstream | 24(47.1) | 7(30.4) | 0.180 |
| Urine | 14(27.5) | 2(8.7) | 0.131 |
| Abdominal | 7(13.7) | 4(17.4) | 0.954 |
| Lung | 35(68.6) | 22(95.7) | 0.011* |
| Skin | 2(3.9) | 0(0) | 0.851 |
| Intracranial | 2(3.6) | 2(8.7) | 0.775 |
| Combined therapy[n(%)] | |||
| Tigecycline | 11(21.6) | 2(8.7) | 0.309 |
| Carbapenem | 6(11.8) | 1(4.3) | 0.562 |
| Colistin/polymyxin B | 2(3.9) | 4(17.4) | 0.132 |
| Aminoglycoside | 7(13.7) | 1(4.3) | 0.425 |
| Phosphomycin | 1(2.0) | 0(0) | 1.000 |
| Metronidazole | 2(3.9) | 0(0) | 0.851 |
表 4
Table 4 Univariate analysis of factors associated with 30-day all-cause mortality
| Risk factors | 30 d survival (n=51) | 30 d mortality (n=23) | P value |
| Basic characteristics | |||
| Age[M(P25, P75)] | 64(46,76) | 71(67,77) | 0.036* |
| BMI[M(P25, P75)] | 22.86(20.81,25.46) | 22.86(20.28,23.88) | 0.139 |
| SOFA[M(P25, P75)] | 6(3,10) | 10(7,12) | 0.001* |
| APACHE Ⅱ[M(P25, P75)] | 17(13,22) | 23(19,26) | <0.001* |
| Male | 44(86.3) | 17(73.9) | 0.335 |
| Medication course[M(P25, P75)] | 11(9,16) | 11(6,14) | 0.064 |
| Combination therapy[M(P25, P75)] | 29(56.9) | 8(34.8) | 0.079 |
| Comorbidities[n(%)] | |||
| Hypertension | 14(27.5) | 3(13.0) | 0.173 |
| Diabetes | 8(15.7) | 5(21.7) | 0.762 |
| COPD | 5(9.8) | 1(4.3) | 0.737 |
| Cardiovascular disease | 23(45.1) | 8(34.8) | 0.405 |
| Malignancy | 7(13.7) | 3(13.0) | 1.000 |
| Liver disease | 14(27.5) | 10(43.5) | 0.173 |
| Kidney disease | 35(68.5) | 19(82.6) | 0.210 |
| ARDS | 12(23.5) | 13(56.5) | 0.005* |
| Severity of illness[n(%)] | |||
| Multisite infections | 25(49.0) | 12(52.2) | 0.802 |
| Septic shock | 26(51.0) | 20(87.0) | 0.003* |
| Usage of vasoactive agent | 24(47.1) | 20(87.0) | 0.001* |
| CRRT | 13(25.5) | 12(52.2) | 0.025* |
| Hours from admission to culture[M(P25, P75)] | 48(24,96) | 48(24,144) | 0.449 |
| Infection sites[n(%)] | |||
| Bloodstream | 24(47.1) | 7(30.4) | 0.180 |
| Urine | 14(27.5) | 2(8.7) | 0.131 |
| Abdominal | 7(13.7) | 4(17.4) | 0.954 |
| Lung | 35(68.6) | 22(95.7) | 0.011* |
| Skin | 2(3.9) | 0(0) | 0.851 |
| Intracranial | 2(3.6) | 2(8.7) | 0.775 |
| Combined therapy[n(%)] | |||
| Tigecycline | 11(21.6) | 2(8.7) | 0.309 |
| Carbapenem | 6(11.8) | 1(4.3) | 0.562 |
| Colistin/polymyxin B | 2(3.9) | 4(17.4) | 0.132 |
| Aminoglycoside | 7(13.7) | 1(4.3) | 0.425 |
| Phosphomycin | 1(2.0) | 0(0) | 1.000 |
| Metronidazole | 2(3.9) | 0(0) | 0.851 |
| Risk factors | B | Standard error | Wald | P value | OR | 95%CI | |
| lower | upper | ||||||
| APACHE Ⅱ | 0.102 | 0.053 | 3.721 | 0.054 | 1.107 | 0.998 | 1.229 |
| Usage of vasoactive agent | 1.975 | 0.759 | 6.773 | 0.009* | 7.205 | 1.628 | 31.883 |
| Age | 0.047 | 0.022 | 4.797 | 0.029* | 1.049 | 1.005 | 1.094 |
表 5
Table 5 Multivariate analysis of factors associated with 30-day all-cause mortality
| Risk factors | B | Standard error | Wald | P value | OR | 95%CI | |
| lower | upper | ||||||
| APACHE Ⅱ | 0.102 | 0.053 | 3.721 | 0.054 | 1.107 | 0.998 | 1.229 |
| Usage of vasoactive agent | 1.975 | 0.759 | 6.773 | 0.009* | 7.205 | 1.628 | 31.883 |
| Age | 0.047 | 0.022 | 4.797 | 0.029* | 1.049 | 1.005 | 1.094 |
| Risk factors | Univariate OR(95%CI) | P value | Multivariate OR(95%CI) | P value |
| Male | 1.079(0.325-3.590) | 0.901 | ||
| Age | 0.944(0.912-0.978) | 0.002* | 0.954(0.918-0.990) | 0.014* |
| SOFA | 0.994(0.898-1.100) | 0.906 | ||
| APACHE Ⅱ | 0.970(0.908-1.036) | 0.371 | ||
| Hours from admission to culture | 0.991(0.984-0.998) | 0.018* | 0.988(0.979-0.998) | 0.014* |
| medication course | 1.083(0.982-1.194) | 0.110 | ||
| Hypertension | 0.474(0.157-1.424) | 0.183 | ||
| Diabetes | 0.103(0.021-0.505) | 0.005* | 0.115(0.020-0.666) | 0.016* |
| COPD | 0.789(0.149-4.196) | 0.781 | ||
| Cardiovascular disease | 0.613(0.241-1.558) | 0.304 | ||
| Malignancy | 0.486(0.125-1.893) | 0.299 | ||
| Liver disease | 0.724(0.272-1.925) | 0.518 | ||
| Kidney disease | 1.023(0.365-2.869) | 0.966 | ||
| ARDS | 0.637(0.241-1.679) | 0.361 | ||
| Multisite infections | 1.116(0.446-2.791) | 0.815 | ||
| Septic shock | 1.127(0.438-2.896) | 0.804 | ||
| Usage of vasoactive agent | 1.151(0.453-2.927) | 0.767 | ||
| CRRT | 0.637(0.241-1.679) | 0.361 | ||
| Combined therapy | 3.467(1.323-9.083) | 0.011* | 4.135(1.225-13.951) | 0.022* |
| Tigecycline | 3.226(0.808-12.879) | 0.097 | ||
| Carbapenem | 2.153(0.390-11.887) | 0.379 | ||
| Colistin/polymyxin B | 0.372(0.064-2.170) | 0.272 | ||
| Aminoglycoside | 6.588(0.767-56.569) | 0.086 |
表 6
Table 6 Univariate and multivariate analysis of factors influencing microbial clearance in patients with CRO infections
| Risk factors | Univariate OR(95%CI) | P value | Multivariate OR(95%CI) | P value |
| Male | 1.079(0.325-3.590) | 0.901 | ||
| Age | 0.944(0.912-0.978) | 0.002* | 0.954(0.918-0.990) | 0.014* |
| SOFA | 0.994(0.898-1.100) | 0.906 | ||
| APACHE Ⅱ | 0.970(0.908-1.036) | 0.371 | ||
| Hours from admission to culture | 0.991(0.984-0.998) | 0.018* | 0.988(0.979-0.998) | 0.014* |
| medication course | 1.083(0.982-1.194) | 0.110 | ||
| Hypertension | 0.474(0.157-1.424) | 0.183 | ||
| Diabetes | 0.103(0.021-0.505) | 0.005* | 0.115(0.020-0.666) | 0.016* |
| COPD | 0.789(0.149-4.196) | 0.781 | ||
| Cardiovascular disease | 0.613(0.241-1.558) | 0.304 | ||
| Malignancy | 0.486(0.125-1.893) | 0.299 | ||
| Liver disease | 0.724(0.272-1.925) | 0.518 | ||
| Kidney disease | 1.023(0.365-2.869) | 0.966 | ||
| ARDS | 0.637(0.241-1.679) | 0.361 | ||
| Multisite infections | 1.116(0.446-2.791) | 0.815 | ||
| Septic shock | 1.127(0.438-2.896) | 0.804 | ||
| Usage of vasoactive agent | 1.151(0.453-2.927) | 0.767 | ||
| CRRT | 0.637(0.241-1.679) | 0.361 | ||
| Combined therapy | 3.467(1.323-9.083) | 0.011* | 4.135(1.225-13.951) | 0.022* |
| Tigecycline | 3.226(0.808-12.879) | 0.097 | ||
| Carbapenem | 2.153(0.390-11.887) | 0.379 | ||
| Colistin/polymyxin B | 0.372(0.064-2.170) | 0.272 | ||
| Aminoglycoside | 6.588(0.767-56.569) | 0.086 |
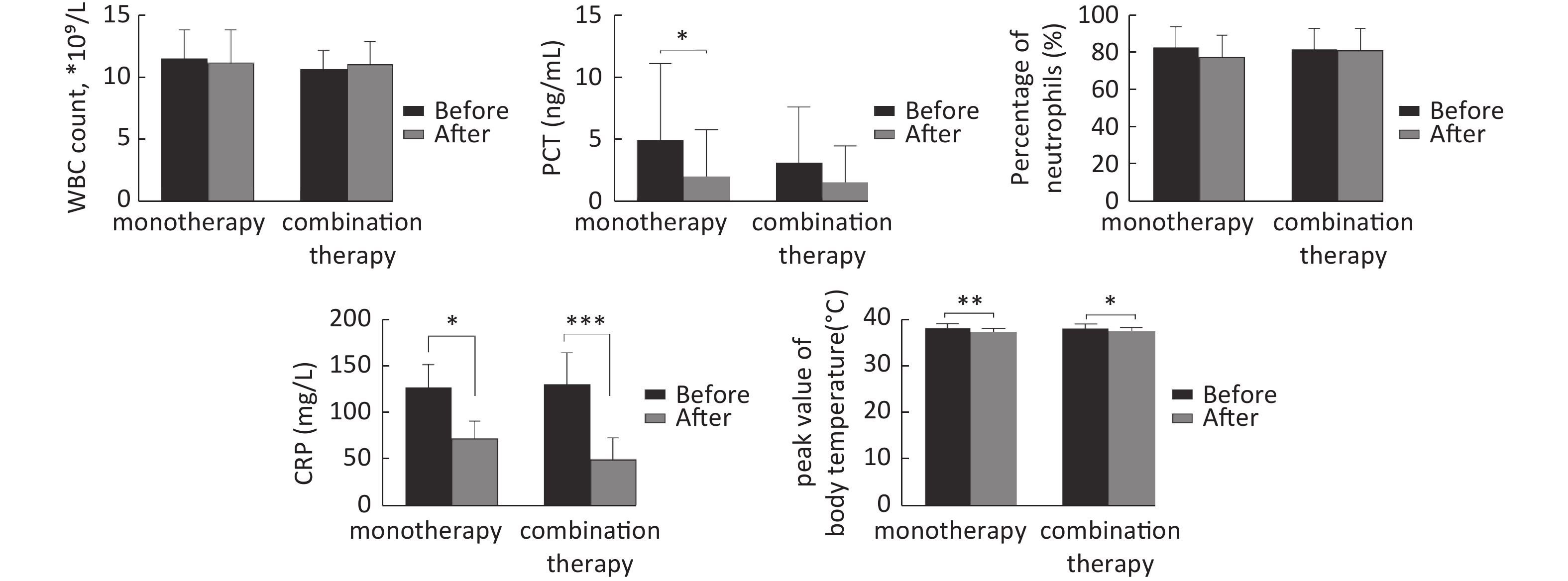
图 1
Fig.1 Changes in infection indicators before and after monotherapy and combination therapy (x?±s, n>3) “Before” refers to data collected within 24 hours before the initiation of CZA, and “After” refers to data collected at the end of the treatment course. *P<0.05, **P<0.01, ***P<0.001, comparison between two groups.
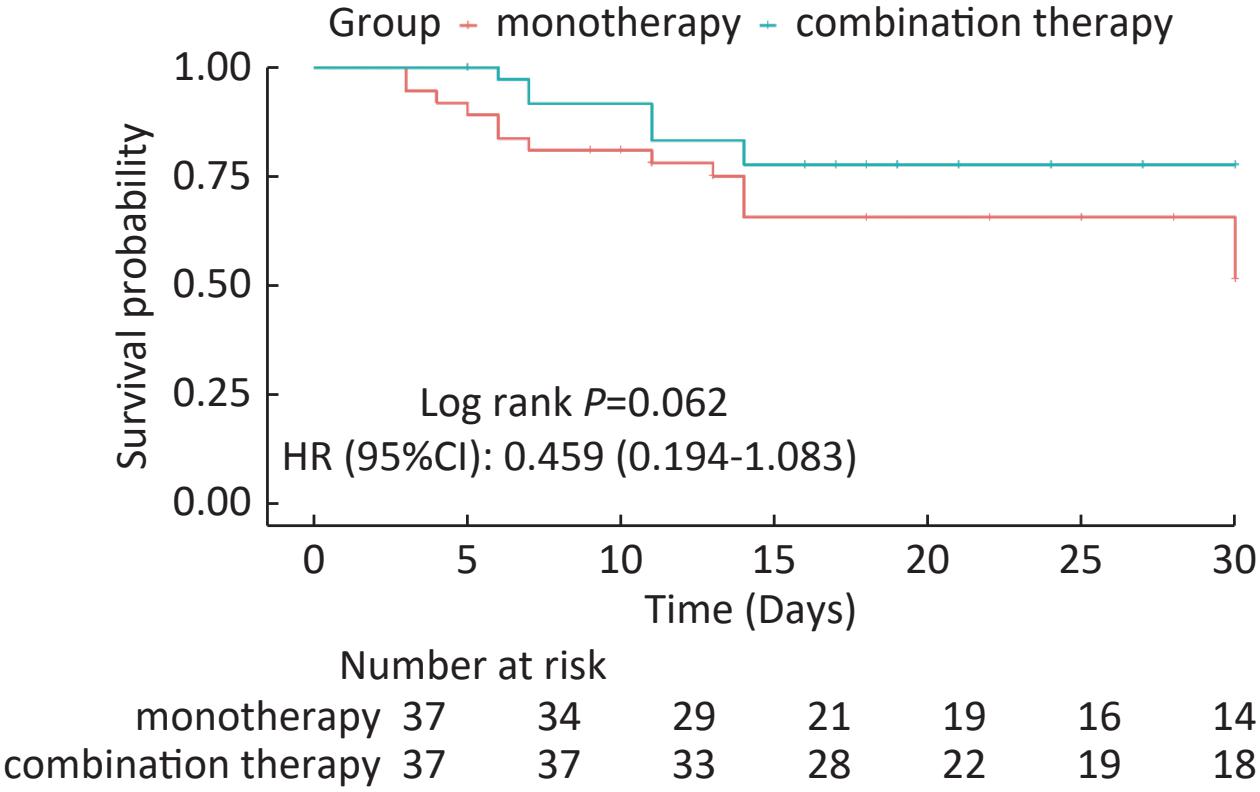
图 2
Fig.2 30-day Kaplan-Meier survival curves
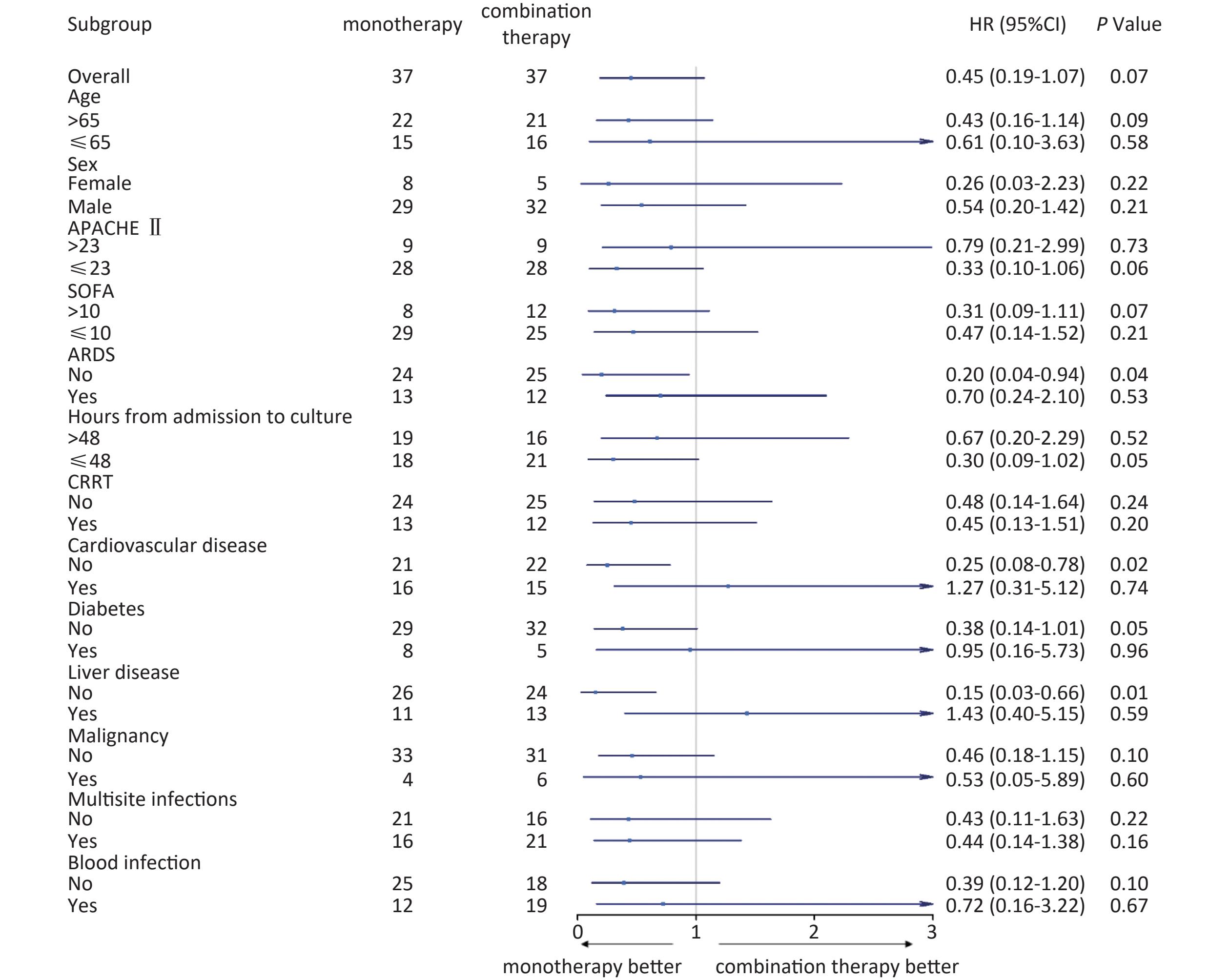
图 3
Fig.3 Subgroup analysis of 30-day all-cause mortality in patients with CRO infections
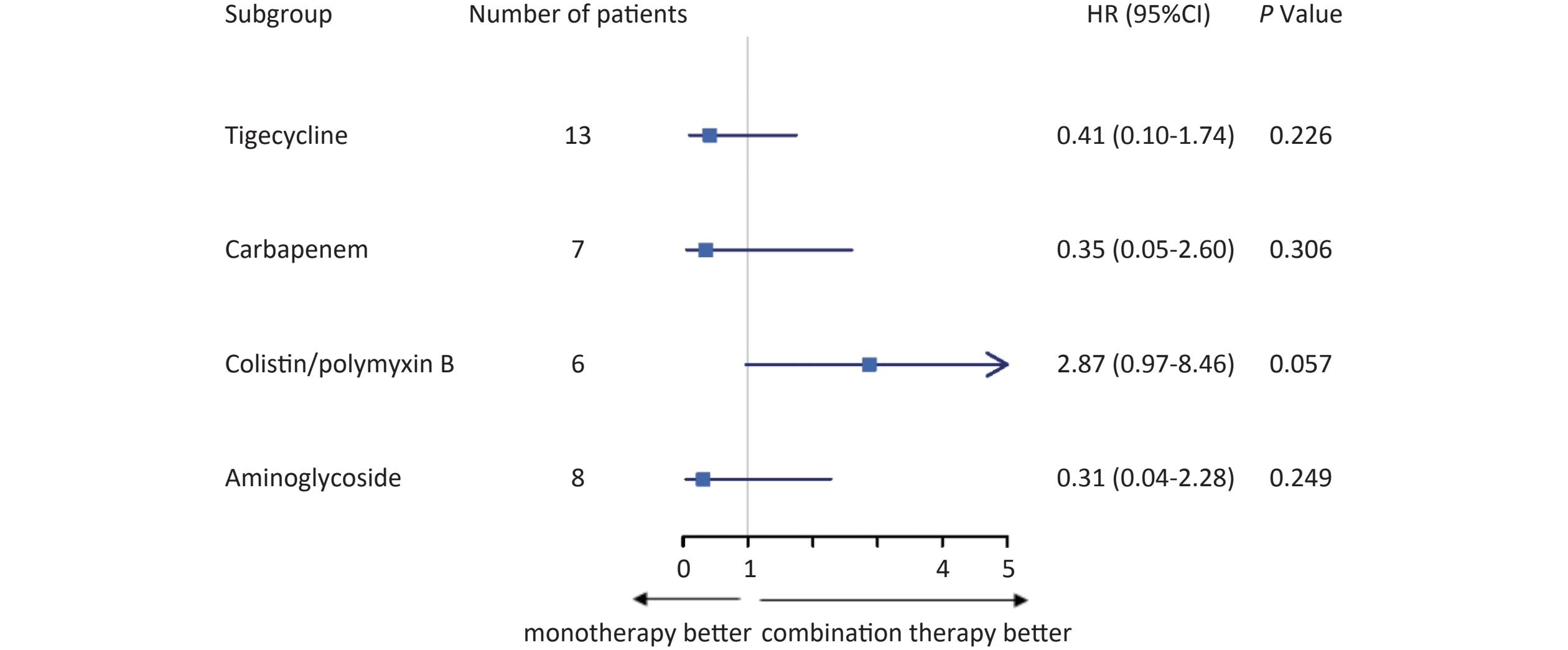
图 4
Fig.4 Subgroup analysis of 30-day all-cause mortality in CRO-infected patients with different therapeutic regimens
| 1 |
Murray CJL, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis[J]. The Lancet, 2022, 399 (10325): 629- 655.
doi: 10.1016/S0140-6736(21)02724-0 |
| 2 |
Lai C, Ma Z, Zhang J, et al. Efficiency of combination therapy versus monotherapy for the treatment of infections due to carbapenem-resistant Gram-negative bacteria: a systematic review and meta-analysis[J]. Syst Rev, 2024, 13 (1): 309.
doi: 10.1186/s13643-024-02695-x |
| 3 | Shields RK, Nguyen MH, Chen L, et al. Ceftazidime-avibactam: a novel cephalosporin/β-lactamase inhibitor combination for the treatment of resistant gram-negative organisms[J]. Clin Infect Dis, 2016, 63 (2): 234- 241. |
| 4 |
Almangour TA, Ghonem L, Aljabri A, et al. Ceftazidime-avibactam versus colistin for the treatment of infections due to carbapenem-resistant enterobacterales: a multicenter cohort study[J]. Infect Drug Resist, 2022, 15, 211- 221.
doi: 10.2147/IDR.S349004 |
| 5 | Tamma PD, Heil EL, Justo JA, et al. Infectious Diseases Society of America 2024 Guidance on the Treatment of Antimicrobial-Resistant Gram-Negative Infections [J]. Clin Infect Dis, 2024: ciae403. |
| 6 |
Liu C, Chen K, Wu Y, et al. Epidemiological and genetic characteristics of clinical carbapenem-resistant Acinetobacter baumannii strains collected countrywide from hospital intensive care units (ICUs) in China[J]. Emerg Microbes Infect, 2022, 11 (1): 1730- 1741.
doi: 10.1080/22221751.2022.2093134 |
| 7 | 《抗菌药物临床试验技术指导原则》写作组. 抗菌药物临床试验技术指导原则[J]. 中国临床药理学杂志, 2014, 30 (9): 844- 856. |
| 8 |
Hetzler LKM, Yuenger V, Micek ST, et al. New antimicrobial treatment options for severe Gram-negative infections[J]. Curr Opin Crit Care, 2022, 28 (5): 522- 533.
doi: 10.1097/mcc.0000000000000968 |
| 9 |
Koulenti D, Song A, Ellingboe A, et al. Infections by multidrug-resistant Gram-negative Bacteria: What's new in our arsenal and what's in the pipeline?[J]. Int J Antimicrob Agents, 2019, 53 (3): 211- 224.
doi: 10.1016/j.ijantimicag.2018.10.011 |
| 10 | Yahav D, Giske CG, Grāmatniece A, et al. New β-lactam-β-lactamase inhibitor combinations[J]. Clin Microbiol Rev, 2020, 34 (1): e00015- 20. |
| 11 |
Neves CS, Moura LCRV, da Costa Lima JL, et al. Clinical outcomes of intensive care unit patients infected with multidrug-resistant gram-negative bacteria treated with ceftazidime/avibactam and ceftolozane/tazobactam[J]. Braz J Microbiol, 2023, 55 (1): 333- 341.
doi: 10.1007/s42770-023-01193-x |
| 12 | King M, Heil E, Kuriakose S, et al. Multicenter study of outcomes with Ceftazidime-Avibactam in patients with Carbapenem-Resistant Enterobacteriaceae infections[J]. Antimicrob Agents Chemother, 2017, 61 (7): e00449- 417. |
| 13 |
Kuloglu TO, Unuvar GK, Cevahir F, et al. Risk factors and mortality rates of carbapenem-resistant Gram-negative bacterial infections in intensive care units[J]. J Intensive Med, 2024, 4 (3): 347- 354.
doi: 10.1016/j.jointm.2023.11.007 |
| 14 |
Jorgensen SCJ, Trinh TD, Zasowski EJ, et al. Real-world experience with ceftazidime-avibactam for multidrug-resistant Gram-negative bacterial infections[J]. Open Forum Infect Dis, 2019, 6 (12): ofz522.
doi: 10.1093/ofid/ofz522 |
| 15 |
Ojdana D, Gutowska A, Sacha P, et al. Activity of ceftazidime-avibactam alone and in combination with ertapenem, fosfomycin, and tigecycline against carbapenemase-producing Klebsiella pneumoniae[J]. Microb Drug Resist, 2019, 25 (9): 1357- 1364.
doi: 10.1089/mdr.2018.0234 |
| 16 |
Liu CW, Chen Q, Ding N, et al. Ceftazidime-avibactam: combination therapy versus monotherapy in the challenge of pneumonia caused by carbapenem-resistant Klebsiella pneumoniae[J]. Heliyon, 2024, 10 (16): e35757.
doi: 10.1016/j.heliyon.2024.e35757 |
| 17 |
Onorato L, Di Caprio G, Signoriello S, et al. Efficacy of ceftazidime/avibactam in monotherapy or combination therapy against carbapenem-resistant Gram-negative bacteria: a meta-analysis[J]. Int J Antimicrob Agents, 2019, 54 (6): 735- 740.
doi: 10.1016/j.ijantimicag.2019.08.025 |
| 18 |
Fiore M, Alfieri A, Di Franco S, et al. Ceftazidime-avibactam combination therapy compared to ceftazidime-avibactam monotherapy for the treatment of severe infections due to carbapenem-resistant pathogens: a systematic review and network meta-analysis[J]. Antibiotics (Basel), 2020, 9 (7): 388.
doi: 10.3390/antibiotics9070388 |
| 19 |
Tumbarello M, Raffaelli F, Giannella M, et al. Ceftazidime-avibactam use for Klebsiella pneumoniae carbapenemase-producing K. pneumoniae infections: a retrospective observational multicenter study[J]. Clin Infect Dis, 2021, 73 (9): 1664- 1676.
doi: 10.1093/cid/ciab176 |
| 20 |
Lin J, Zhang L, Zhou M, et al. Combination therapy of ceftazidime/avibactam for the treatment of patients infected with carbapenem-resistant Klebsiella pneumoniae: a multicenter retrospective study[J]. Infect Dis Ther, 2023, 12 (8): 2165- 2177.
doi: 10.1007/s40121-023-00852-8 |
| 21 |
Aslan AT, Ezure Y, Horcajada JP, et al. In vitro, in vivo and clinical studies comparing the efficacy of ceftazidime-avibactam monotherapy with ceftazidime-avibactam-containing combination regimens against carbapenem-resistant Enterobacterales and multidrug-resistant Pseudomonas aeruginosa isolates or infections: a scoping review[J]. Front Med (Lausanne), 2023, 10, 1249030.
doi: 10.3389/fmed.2023.1249030 |
| 22 |
Carrara E, Bodo D, Tacconelli E. Combination versus monotherapy for the treatment of infections due to carbapenem-resistant Enterobacteriaceae[J]. Curr Opin Infect Dis, 2018, 31 (6): 594- 599.
doi: 10.1097/QCO.0000000000000495 |
| 23 |
Hsu WC, Tsai WW, Lai CC, et al. Ceftazidime-avibactam combination therapy versus monotherapy for treating carbapenem-resistant gram-negative infection: a systematic review and meta-analysis[J]. Infection, 2024, 52 (5): 2029- 2042.
doi: 10.1007/s15010-024-02277-y |
| 24 |
Zhong H, Zhang X, Zhang Z, et al. Evaluation of the efficacy and safety of ceftazidime/avibactam in the treatment of Gram-negative bacterial infections: a systematic review and meta-analysis[J]. Int J Antimicrob Agents, 2018, 52 (4): 443- 450.
doi: 10.1016/j.ijantimicag.2018.07.004 |
| 25 |
Park BD, Faubel S. Acute kidney injury and acute respiratory distress syndrome[J]. Crit Care Clin, 2021, 37 (4): 835- 849.
doi: 10.1016/j.ccc.2021.05.007 |
| 26 |
Borges A, Bento L. Organ crosstalk and dysfunction in sepsis[J]. Ann Intensive Care, 2024, 14 (1): 147.
doi: 10.1186/s13613-024-01377-0 |
| 27 |
Dartiguelongue J, Borges M. Systemic inflammation and sepsis. Part I: Storm formation[J]. Arch Argent Pediatr, 2020, 118 (6): e527- e535.
doi: 10.5546/aap.2020.eng.e527 |
| 28 |
Torres LK, Pickkers P, van der Poll T. Sepsis-induced immunosuppression[J]. Annu Rev Physiol, 2022, 84, 157- 181.
doi: 10.1146/annurev-physiol-061121-040214 |
| 29 |
Lu J, Meng Y, Cao Z, et al. Efficacy of ceftazidime-avibactam with or without polymyxin for carbapenem-resistant Klebsiella pneumoniae infections after initial treatment with polymyxin[J]. Microbiol Spectr, 2025, 13 (1): e0177024.
doi: 10.1128/spectrum.01770-24 |
| 30 | Zhuang HH, Qu Q, Long WM, et al. Ceftazidime/avibactam versus polymyxin B in carbapenem-resistant Klebsiella pneumoniae infections: a propensity score-matched multicenter real-world study[J]. Infection, 2024, 53 (1): 95- 106. |
| 31 |
Zhang F, Li P, Zhong J, et al. Clinical outcomes and risk factors for mortality in recipients with carbapenem-resistant gram-negative bacilli infections after kidney transplantation treated with ceftazidime-avibactam: a retrospective study[J]. Front Cell Infect Microbiol, 2024, 14, 1404404.
doi: 10.3389/fcimb.2024.1404404 |
| 32 |
Dumlu R, Sahin M, Derin O, et al. Ceftazidime-avibactam versus polymyxin-based combination therapies: a study on 30-day mortality in carbapenem-resistant Enterobacterales bloodstream infections in an OXA-48-endemic region[J]. Antibiotics (Basel), 2024, 13 (10): 915.
doi: 10.3390/antibiotics13100990 |
| 33 |
Wang Z, Saxena A, Yan W, et al. The impact of aging on neutrophil functions and the contribution to periodontitis[J]. Int J Oral Sci, 2025, 17 (1): 10.
doi: 10.1038/s41368-024-00332-w |
| 34 |
Thimmappa PY, Vasishta S, Ganesh K, et al. Neutrophil (dys)function due to altered immuno-metabolic axis in type 2 diabetes: implications in combating infections[J]. Hum Cell, 2023, 36 (4): 1265- 1282.
doi: 10.1007/s13577-023-00905-7 |
| 35 | Paudel S, John PP, Poorbaghi SL, et al. Systematic review of literature examining bacterial urinary tract infections in diabetes[J]. J Diabetes Res, 2022, 2022, 3588297. |
| 36 |
Shook JC, Garcia C, Darwitz BP, et al. Diabetes potentiates the emergence and expansion of antibiotic resistance[J]. Sci Adv, 2025, 11 (7): eads1591.
doi: 10.1126/sciadv.ads1591 |
| 37 |
Semet C, Efe K, Akalın H, et al. Outcome of carbapenem or colistin resistant Klebsiella pneumoniae bacteremia in the intensive care unit[J]. Sci Rep, 2024, 14 (1): 25805.
doi: 10.1038/s41598-024-73786-x |
| 38 |
Bassetti M, Kanj SS, Kiratisin P, et al. Early appropriate diagnostics and treatment of MDR Gram-negative infections[J]. JAC Antimicrob Resist, 2022, 4 (5): dlac089.
doi: 10.1093/jacamr/dlac089 |
| 39 |
Sousa A, Pérez-Rodríguez MT, Soto A, et al. Effectiveness of ceftazidime/avibactam as salvage therapy for treatment of infections due to OXA-48 carbapenemase-producing Enterobacteriaceae[J]. J Antimicrob Chemother, 2018, 73 (11): 3170- 3175.
doi: 10.1093/jac/dky295 |
| 40 |
Yang MC, Wu YK, Lan CC, et al. Antibiotic stewardship related to delayed diagnosis and poor prognosis of critically ill patients with vancomycin-resistant enterococcal bacteremia: a retrospective cohort study[J]. Infect Drug Resist, 2022, 15, 723- 734.
doi: 10.2147/IDR.S354701 |
| 41 |
Kengkla K, Wongyingsin M, Chaomuong N, et al. Clinical and economic outcomes attributable to carbapenem-resistant Enterobacterales and delayed appropriate antibiotic therapy in hospitalized patients[J]. Infect Control Hosp Epidemiol, 2022, 43 (10): 1349- 1359.
doi: 10.1017/ice.2021.446 |
| 42 | 朱勋帅, 王海妮, 郭凯欣. 头孢他啶/阿维巴坦挽救性治疗多重耐药革兰阴性菌感染患者的临床特征和结局——一项回顾性病例分析[J]. 中国中西医结合急救杂志, 2022, 29 (3): 284- 287. |
| 43 |
Castón JJ, Lacort-Peralta I, Martín-Dávila P, et al. Clinical efficacy of ceftazidime/avibactam versus other active agents for the treatment of bacteremia due to carbapenemase-producing Enterobacteriaceae in hematologic patients[J]. Int J Infect Dis, 2017, 59, 118- 123.
doi: 10.1016/j.ijid.2017.03.021 |
| No related articles found! |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||


